AI in claim adjudication is the under-discussed health-AI win the prior-auth mandate is about to mainstream.
The trade-press attention on AI in healthcare has concentrated on the diagnostic-class deployments (radiology imaging, dermatology screening, cardiology rhythm analysis) and on the patient-facing chatbot deployments. The under-discussed deployment that has been running quietly at scale for several years is claim adjudication. U.S. payers have been deploying ML models on incoming claims for fraud detection, routing optimization, and prior-authorization processing since at least 2018, with substantial expansion through 2022-2025. The aggregated revenue-and-cost-line impact across the major payers exceeds the impact of every diagnostic-AI tool combined by a substantial margin.
The 2024-2025 federal-and-state regulatory trajectory on prior-authorization response times is about to mainstream the deployment further. The CMS prior-auth interoperability rule that progressively binds through 2026-2027 requires payers to respond to prior-auth requests on tighter timelines, with substantial technical-and-operational requirements that the manual-review-only payers cannot meet at the volume the rule implies. The mandate is, in operational terms, a forcing function for accelerated AI deployment in the claim-adjudication-and-prior-auth layer.
This explainer walks what claim-adjudication AI actually does, why it is more revenue-impactful than diagnostic-AI in aggregate, the prior-auth-mandate dynamics that are accelerating it, and what the durable read on the deployment trajectory should be.
What claim-adjudication AI actually does
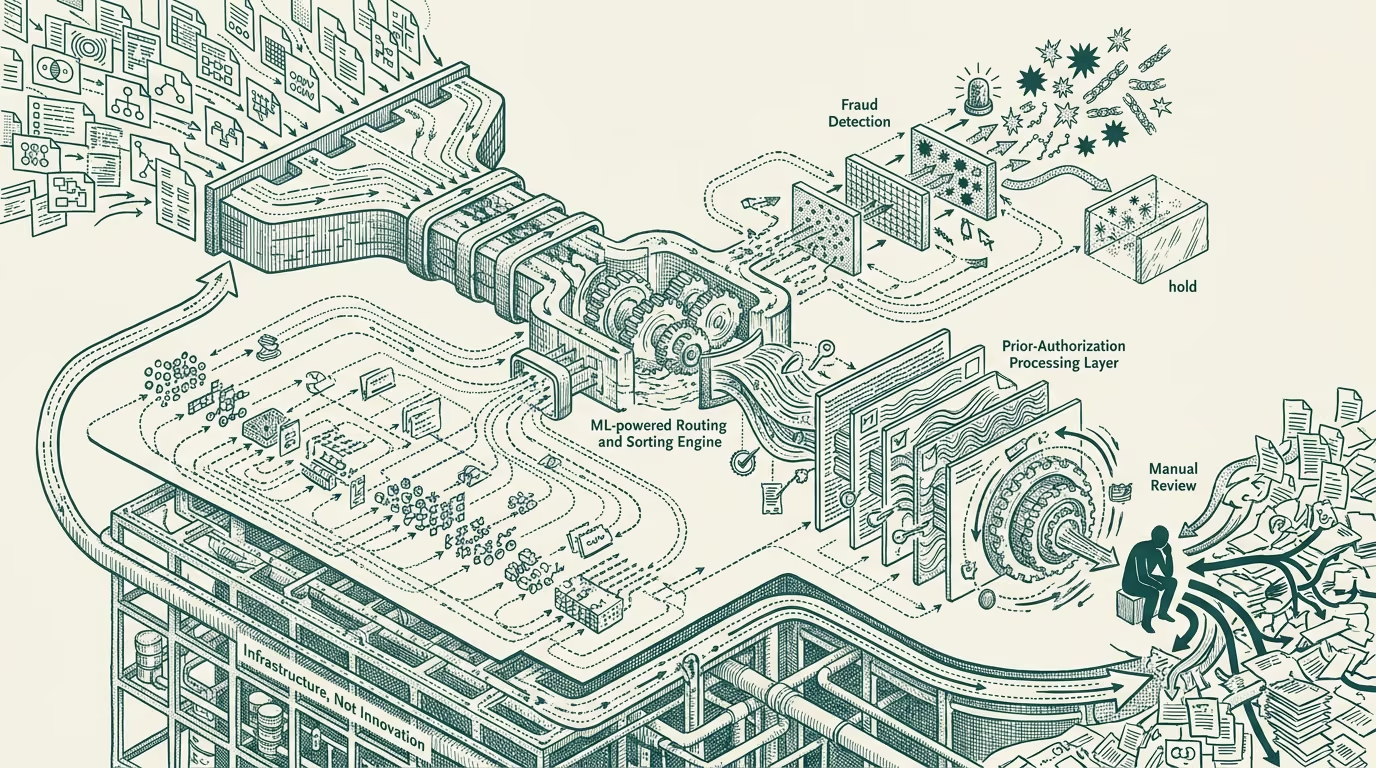
The claim-adjudication-AI category covers several specific deployments at the U.S. payer-class.
The fraud-and-abuse detection layer runs ML models on incoming claims to identify patterns consistent with fraudulent billing, upcoding, unbundling of services, duplicate-claim submission, and the various other patterns that payer special-investigations units have historically detected through manual review. The AI deployment processes substantially higher volume than the manual-review infrastructure could, with substantially better recall on the established fraud patterns and modestly better precision on the novel-pattern detection.
The routing-and-priority layer routes incoming claims through the payer's processing pipeline based on the model's assessment of the claim's complexity, risk, and likelihood of requiring human review. Simple claims that match standard patterns route through automated processing. Complex or anomalous claims route to human review. The routing optimization saves substantial human-review capacity that the payer can redeploy to the harder claims.
The prior-authorization processing layer runs ML models against incoming prior-auth requests to identify the requests that match clear-approval patterns (where the model can recommend automatic approval based on clinical-and-policy guidelines), clear-denial patterns (where the model can recommend automatic denial with explanation), and ambiguous patterns (which route to human clinical review). The deployment substantially compresses the prior-auth processing time for the clear-approval-and-denial categories.
The duplicate-and-coordination-of-benefits detection layer runs ML models against incoming claims to identify claims that are duplicates of prior submissions, that should be routed to a different payer (Medicare-as-secondary, commercial-as-primary configurations), or that involve coordination questions the payer's automated processing should resolve before the claim flows downstream.
The combined deployment across these four layers handles a substantial fraction of the U.S. payer-class claim volume, with the AI-augmented processing producing both cost savings and revenue protection in the major-payer P&Ls.
Why it is more revenue-impactful than diagnostic-AI
The aggregate revenue-and-cost-line impact of claim-adjudication AI exceeds diagnostic-AI by a substantial margin for several reasons.
The volume is substantially larger. The U.S. payer system processes billions of claims annually. The diagnostic-AI deployments touch hundreds of millions of patient-encounters annually. The volume difference produces aggregate-impact differences even when the per-unit impact of diagnostic-AI is larger.
The per-unit dollar impact is also meaningful at the claim-adjudication layer. A correctly-detected fraudulent claim saves the payer the claim's full value, which can run into thousands or tens of thousands of dollars per detection. A correctly-routed simple claim saves the human-review-cost, which is meaningful at scale. A correctly-processed prior-auth saves the cycle-time-and-staffing-cost the payer would otherwise absorb.
The unit economics for the payer are also substantially better than the diagnostic-AI economics for the deploying clinical institution. The claim-adjudication AI runs against the payer's existing claims-processing infrastructure, with the AI deployment substituting for human-review labor that the payer was already paying. The diagnostic-AI runs alongside the existing clinical workflow, often as augmentation rather than substitution, with the per-clinical-encounter unit-economics being smaller.
The combined effect is that the major U.S. payers are, in operational terms, the heaviest production-AI deployers in healthcare, with budgets and engineering investment that exceed what the headline diagnostic-AI vendors collectively command. The trade-press coverage has been generally not surfacing this because the payer-side deployment is operationally invisible to the consumer and to the press in a way the diagnostic-AI deployments are not.
The prior-auth-mandate dynamics
The CMS prior-authorization interoperability rule that progressively binds through 2026-2027 sets specific response-time requirements that the major payers must meet for prior-auth requests in the Medicare and Medicaid populations. The requirements include a 7-day standard for non-urgent requests and a 72-hour standard for urgent requests, with the requirements applying to a substantial share of the payer-class claim volume.
The technical-and-operational requirements for meeting the rule include API-based prior-auth submission, machine-readable prior-auth status, and the underlying processing infrastructure capable of producing decisions within the timelines. The combination implies AI-augmented processing because manual-review-only operations cannot meet the volume-at-the-timeline.
The mandate is, in operational terms, a forcing function. Payers that have not deployed substantial prior-auth-processing AI through 2024-2025 are running into the deadline with operational gaps. Payers that have deployed substantial AI through this period are positioned to meet the rule with margin to spare. The differential operational position is going to surface in the next 12-24 months as the rule binds and the laggard payers absorb the cost of catching up.
What the operator class should take from this
For founders building healthcare-AI products in 2025-2026, the operator-class read is that the payer-side claim-adjudication-and-prior-auth layer is one of the larger near-term opportunities, with the mandate-driven acceleration making the buyer urgency higher than it has been at any prior moment in the category. Vendors who can ship products that integrate with the payer's claim-adjudication infrastructure or that help the payer meet the prior-auth mandate are operating with strong tailwinds.
For investors evaluating healthcare-AI through 2025-2026, the read is that the claim-adjudication category is under-priced relative to its actual revenue-impact and growth trajectory. The investment-class allocation has concentrated on the diagnostic-AI category and the consumer-facing AI category, which are smaller and more competitively-dense than the claim-adjudication category.
For payers reading the mandate trajectory, the part that holds is that the prior-auth-AI deployment is no longer optional and the timeline for catching up is short. Payers without substantial deployment through 2025 will be in operational distress through 2026-2027 as the mandate binds.
The under-discussed AI-in-healthcare deployment is in claim adjudication. The mandate is about to make it the most-discussed deployment. The operator-grade building or investing in this space has tailwinds that the trade-press coverage has not yet caught up to. Build accordingly. The next 18-24 months will move the category from quiet-deployment to visible-deployment, and the early movers will be substantially ahead of the entrants who arrive after the trade press notices.
—TJ